1. Invests in the acquisition of evidence through participation in workshops, continued education and pursuit of additional degrees.
During my LeBonheur rotation, I attended three in-service presentations which discussed gastric-tube management and care, tracheostomy management and care, and Ehlers-Danlos Syndrome (EDS). These in-services covered precautions and things to look out for during treatment sessions, what to do in case of emergency, and general information on diagnoses. Below is the title page for the in-service presentation on EDS.
2. Is a knowledgeable consumer of global research related to occupational therapy and utilizes an evidence based approach to practice.
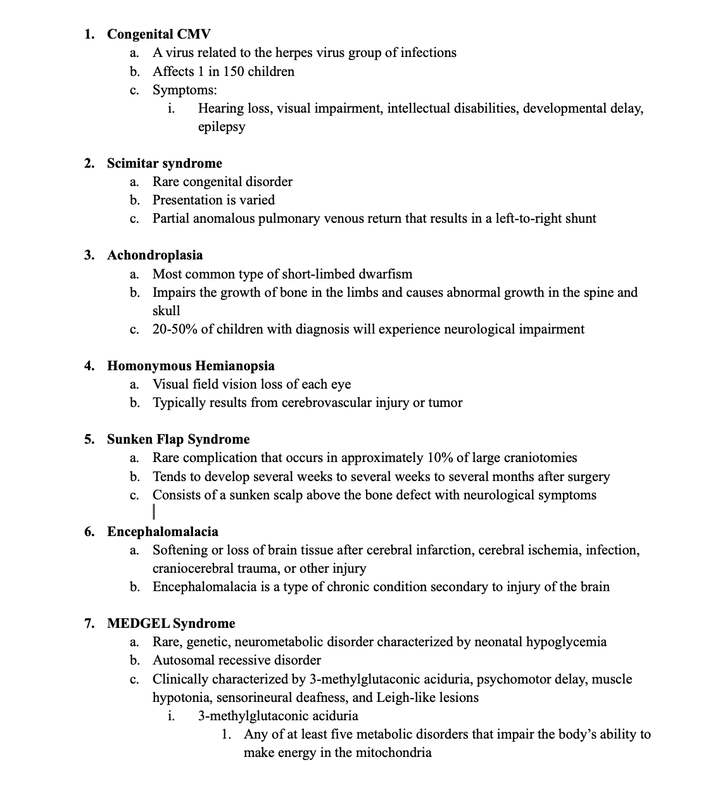
At my first level II rotation in outpatient pediatrics, I came across many patients that had a diagnosis that I was not familiar with. During my free time at work, I would research these diagnoses in order to better understand my patients and how I could best serve them. I created a document with a list of these diagnoses, their physiology, and how they typically present. This document not only helped me grow my knowledge of pediatric diagnoses, but also helped me in the evaluation process and the implementation of interventions. Pictures of this document are below.
3. Integrates individual clinical expertise and patient values with the best available external clinical evidence.
Early mobility in acute care is something that therapists, nurses, and doctors frequently talk about. Incorporating mobility early into the rehabilitation process leads to greater chances of recovery. There was recently a study completed at Baptist Memorial that focused on early mobility in acute care. The results of the study showed shorter hospital stays and faster recovery overall. Many patients that I worked with were independent prior to being admitted to the hospital, and they wanted to return to that independence. I combined external clinical evidence as well as patient values in order to provide the best care possible to all of my patients.
4. Applies the domain of occupational therapy in gathering, evaluating, setting goals, planning and implementing occupational therapy.
During my rotation at Baptist Memorial Hospital, I was able to apply all of the domains of occupational therapy. I mainly completed the evaluations of the patients that I saw. I would complete a thorough chart review, evaluate the patient, and create appropriate goals. My fieldwork educator would frequently assign me to see the patients that I evaluated for treatments as well. I was able to implement my interventions and work towards the goals I created with my patients. With every patient that I saw, I would also make discharge recommendations and DME recommendations.
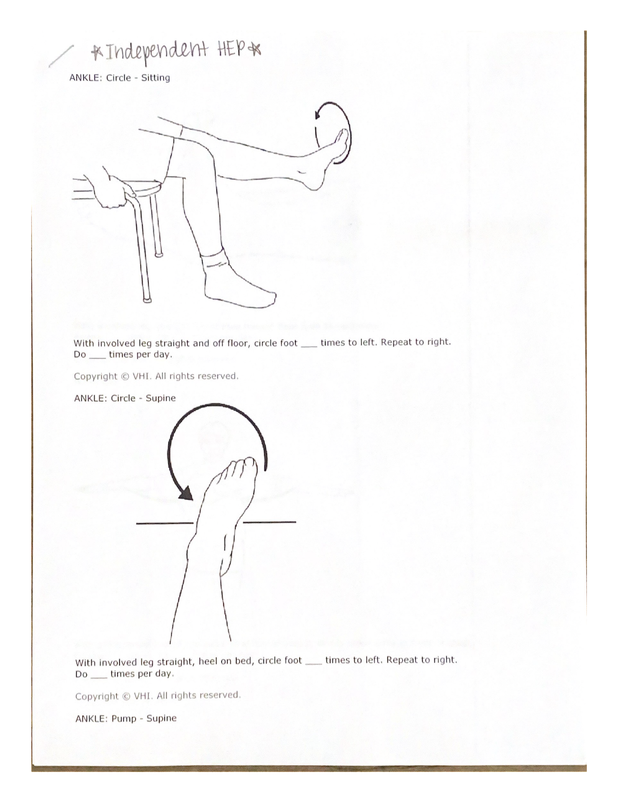
5. Contributes to the knowledge base of OT practice by mentoring students, performing research, publishing, presenting, and/or teaching.
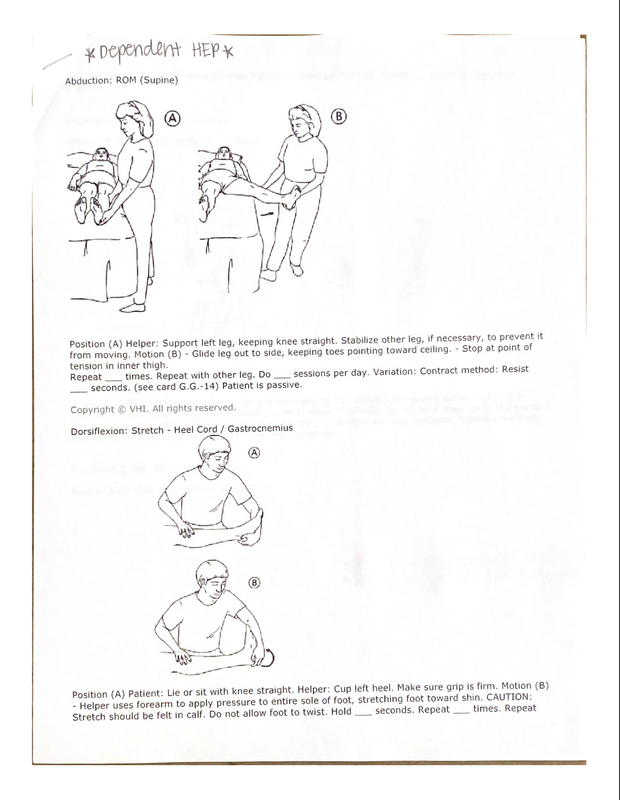
For my student project at Baptist, I created a HEP for patients that occupational therapy were not going to follow while they were in the hospital. These patients were signed off on because they were either independent or dependent during the evaluation. The therapy directors at Baptist said that a HEP needed to be created in order to give patients and patient's families something to work on since occupational therapy was not going to follow up with them. The HEP that I created for dependent patients mainly consisted of passive range of motion as well as bed mobility. The HEP that I created for independent patients focused on active range of motion as well as balance and functional mobility. I presented these HEPs to the therapy department and left a copy with them to give to patients that they were signing off on as well.
6. Incorporates continues education as a lifelong practice with the commitment to remain up-to-date and well-informed.
While at my acute care rotation, I attended an in-service presentation that discussed discharge recommendations and how to work as a team with the case managers in order to make the best recommendations for our patients.

